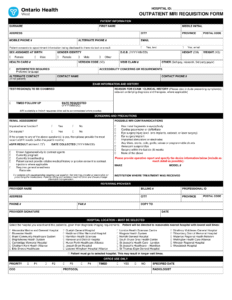
Visit wecare2image.ca to obtain the requisition. Please do not fax the form to Hamilton Family Health Team.
File Type:
www
Downloads:
1082
Visit wecare2image.ca to obtain the requisition. Please do not fax the form to Hamilton Family Health Team.